Muscle Imbalances and Scoliosis (2018 Updates Below)
Muscle imbalances and scoliosis go hand-in-hand. For scoliosis, exercise often aims at making tight muscles more flexible and weak muscles stronger. However, this approach is simplistic and does not take into account the complexity of the changes that occur with scoliosis.
Scoliosis Syndrome TASK: To identify a predictable pattern of tight to weak muscles in 4-Curve Scoliosis.
Introduction
Vladimr Janda (1928-2002) found muscle imbalances to be “systematic and predictable” due to the innate function of the sensori-motor system. Janda further suggested a strong relationship between joint dysfunction and muscle imbalance (Source: Janda 1986a). He identified a predictable pattern of muscle tightness and weakness in his Upper and Lower Crossed Syndromes.

In the image, the girl on the left shows a normal posture. The girl on the right shows Janda’s “Upper Crossed Syndrome”. In this syndrome there is a predictable pattern of weak and tight muscles
| Weak | Tight |
|---|---|
| Scalenes | Pectorals |
| Lower Trapezius | Upper Trapezius |
In Scoliosis, there also appears to be a predictable tight and weak muscle pattern. These predictable muscle pattern changes are concurrent with defined scoliosis skeletal patterns. The defined skeletal pattern used for this study is a 4-Curve Scoliosis.
The 4-curve Scoliosis (Source: Schroth) pattern includes:
- Cervical curve with the convexity to the left. Shoulder girdle glides left.
- Thoracic curve with the convexity to the right.
- Lumbar curve with the convexity to the left.
- Pelvic compensation with an L5-S1 change to the right and a coccyx that terminates pointing left.
PURPOSE: To find if muscle imbalances and scoliosis create predictable patterns.
If a predictable muscle pattern is found then a specific method of management through exercise can be assigned.
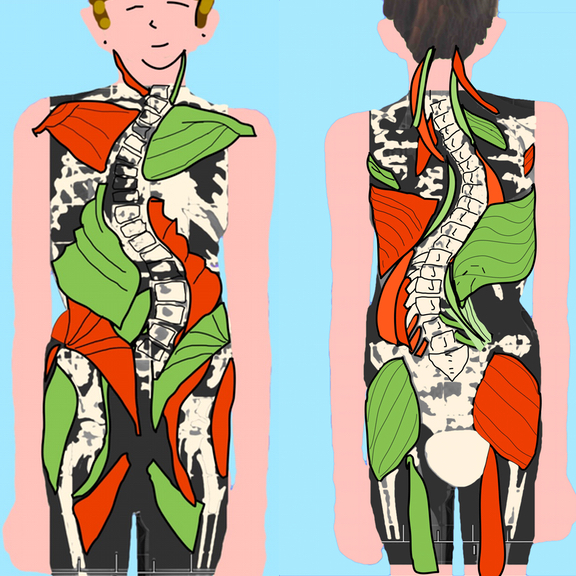
Patterns of Muscle Imbalance found so far:
- Green is Weak/Inhibited
- Red is Tight/Facilitated

Within a typical 4-curve scoliosis, we have found the following muscles imbalances.
We have found theses muscles to be generally inhibited:
Gluteus maximus – Left
Hamstrings – Left
Quadratus Lumborum – Right
Latissimus Doris – Right
Rhomboids – Right
Serratus Anterior – Left
Levator Scapula – Left
We have found theses muscles to be generally facilitated:
Gluteus maximus – Right
Hamstrings – Right
Quadratus Lumborum – Left
Latissimus Doris – Left
Rhomboids – Left
Serratus Anterior – Right
Levator Scapula – Right
Study continues on muscle imbalances and scoliosis to see if a predictable pattern of muscle imbalances occurs within certain predictable patterns of change associated with scoliosis.
Scoliosis Syndrome Updated 2018
A lot has changed since this project began in 2014. I can no longer think of the asymmetries of the spine as weak or strong, facilitated or inhibited. This change in thinking comes not only from working with scoliosis clients but also as a result of performing two scoliosis dissections.
At one dissection, a fellow student walked by the scoliosis cadaver we were working on and remarked, “This woman is Buff!” Meaning, this woman, as tiny as she was, appeared very, very strong. The muscles throughout her spine were strong and defined and hypertrophied. Yes, some were living in a shape that was longer or shorter than physiologically normal, but all of the muscles were very toned. Possibly too toned: hypertonic. Even in death the muscles were taut, like strings on a banjo (or cello, if you are more sophisticated than I). So what side was weak? I couldn’t see one. And what side was strong? Well… They all appeared strong. They all appeared to have the perfect strength (for better or worse) to hold the position of her scoliosis. And it wasn’t just the muscles that were long and short, it was everything. Veins, arteries, nerves, organs, connective tissue, bones… everything had changed to fit the scoliosis.
It is with every step of learning, that the Scoliosis Syndrome continues to change. I welcome your input and your collaboration. Email me!
In the meantime, what you see below is a sampling of our findings. And they continue to grow.
Double Major Curve
Cervical spine
Shoulder Girlde
Thoracic Spine and Thorax
Lumbar Spine
Pelvis
Physiologically Short
(R) Sternocleidomastoid
(R) Levator Scapulae|
(R) Cervicis Longus
________________
(R) Pectoralis Major and Minor
(R) Anterior Deltoid
(R) Coracobrachialis
(R) Teres Major
_______________
(L) Rhomboid
(R) Latissimus Dorsi
(L) External Oblique
(R) Internal Oblique
(R) Fibers of Diaphragm
________________
R & L Thoraco-lumbar fascia thickened
(R) medial portion of quadratus lumborum
(L) Thin layer of superficial fascia
_______________
(R) Gluteus maximus
(L) Gluteus minimus/medius
(R) Psoas
(L) Iliacus
Physiologically Long
(L) Sternocleidomastoid
(L) Levator Scapulae
(R) Cervicis Longus
___________________
(L) Pectoralis Major and Minor
(L) Posterior Deltoid
(L) Coracobrachialis
(L) Teres Major
_______________
(R) Rhomboid
(L) Latissimus Dorsi
(R) External Oblique
(L) Internal Oblique
(L) Fibers of Diaphragm
________________
R & L Thoraco-lumbar fascia thickened
(L) medial portion of quadratus lumborum
(R) thick layer of superficial fascia giving the (R) lumbar concavity its softer texture
_______________
(L) Gluteus maximus
(R) Gluteus minimus/medius
(L) Psoas
(R) Iliacus
What Comes Next
Understanding scoliosis as a whole-body adaptation naturally leads to deeper questions—about movement, flexibility, aging, and even long-term health beyond the spine.
In Scoliosis Syndrome, Part 2, we explore what this understanding means in practice: how exercise needs to change, why stretching must be specific, and how scoliosis can influence the body over time.
Continue reading: Scoliosis Syndrome, Part 2 – How Scoliosis Affects Movement, Flexibility, and Aging